
Helpful resources and clinical insights
Access resources for use in your practice
Patient Symptom Fact Sheet

Download this fact sheet to review the spectrum of polycythemia vera (PV) symptoms and how they burden the daily lives of people with PV.
Patient Discussion Guide
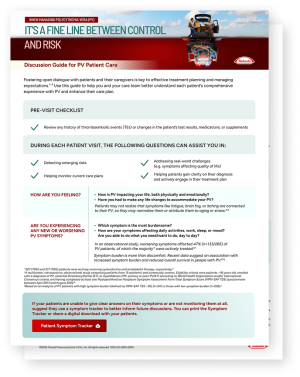
Use this guide to help you and your care team better understand each patient’s comprehensive experience with PV and enhance their care plan.
Patient Symptom Tracker
Share this resource with your patients so they can track their symptoms over time. At their next appointment, review the completed symptom tracker together so you can focus on the symptoms that affect them the most.
PV Summary Guide

This real-world evidence summary highlights the ongoing challenge of maintaining HCT below 45% in people with PV, along with the impacts of persistent symptom burden and iron dysregulation.
Hear insights from a KOL and a real
patient with PV
Hear about PV from a KOL
Hear a KOL discuss a variety of PV topics, including patient diagnosis, current treatment strategies, and the impact of iron dysregulation.
ViewHide Transcript
0:06: Hello and welcome to today's expert discussion about polycythemia vera or PV.
0:12: I'm Doctor Abdulraheem Yacoub, a physician and professor of hematological malignancies and cellular therapeutics at the University of Kansas Medical Center.
0:21: In this video, we will explore important aspects of PV including disease biology, the symptoms and emotional burden patients may experience, and key clinical considerations that can influence how we manage patients.
0:37: And I'm Doctor Jennifer Vaughn, a hematologist-oncologist, and associate professor of hematology at Ohio State University.
0:45: Let's get started.
0:48: Polycythemia vera is a chronic malignancy where the immediate danger stems from the overproduction of red blood cells which creates inefficient hyper viscous blood flow.
1:01: The disease is driven by acquired mutations.
1:04: 97% to 98% of patients with PV have a mutation in the Janus kinase 2 or JAK-2 gene, with the vast majority of those having the V617F mutation.
1:17: I tell my patients that when that mutation occurs, it is like flipping a light switch on permanently, and the JAK2-driven growth signaling pathway increases production of red blood cells.
1:30: Yes, the JAK2 mutation leads to continuous firing of the pathway, driving nonstop overproduction of blood elements, whether the body physiologically needs that or not.
1:42: The resulting red blood cell mass and blood viscosity lead to chronic symptoms such as headaches, fatigue, pleuritis, erythromyalgia, and cognitive fog.
1:53: More importantly, it substantially increases the risk of thrombotic complications, including deep vein thrombosis, pulmonary embolism, heart attack, and stroke.
2:05: A major contributor to thrombotic events is uncontrolled hematocrit at or above 45%.
2:13: At that threshold, blood viscosity and red blood cell mass increase enough to reduce microvascular flow.
2:20: That's where we begin to see real clinical risks emerge.
2:25: Around 40% of patients experience thrombotic events after diagnosis.
2:31: These events are some of the leading drivers of morbidity and mortality in PV.
2:39: Yes, and clinical data demonstrate how even slight increases in hematocrit can drastically increase risk.
2:46: In the cytopPV study, people with PV who consistently maintained hematocrit levels greater than or equal to 45%, specifically within 45% to 50%, were 4 times more likely to experience major thrombotic events or cardiovascular death than those whose hematocrit was tightly controlled below the 45% threshold.
3:09: A substantial number of patients still spend significant time with uncontrolled hematocrit despite treatment, highlighting the need for more proactive approaches for managing patients with PV.
3:23: Most patients with PV are diagnosed incidentally.
3:27: They visit their primary care physician for routine blood work, and an elevated hemoglobin or hematocrit raises the first concern.
3:36: But that's not always how it happens.
3:39: About 30% of patients are first identified after a thrombotic event, such as a heart attack or stroke.
3:46: PV is a potentially life threatening disease, yet its symptoms may go underrecognized.
3:54: This figure from the MPN Landmark survey reflects what I see in my practice, where common symptoms include fatigue, itching, night sweats, concentration problems, abdominal discomfort, and inactivity.
4:09: What do you think, Doctor Vaughn?
4:12: In my clinical experience, patients with PV often think they are asymptomatic, but when I probe further, I find they're experiencing significant symptom burden.
4:24: The symptoms fall into three main categories, hyperviscosity symptoms such as headaches and visual changes, microvascular symptoms such as erythromyalgia, and inflammatory symptoms such as itching.
4:36: Patients experience significant amounts of fatigue, which is often multifactorial related to inflammation and iron deficiency.
4:45: This makes sense when we consider that their bodies have been in overdrive, producing excess red blood cells and depleting their natural iron stores.
4:55: So let's move into a discussion about how we treat these patients.
4:59: In clinical practice, we still stratify patients with PV into low and high risk groups based on two key factors age and history of thrombosis.
5:10: But regardless of this stratification, the main pillar of treating PV is to maintain hematocrit consistently below 45%.
5:19: That can't be emphasized enough.
5:23: Yes, of course, my immediate priority in PV is targeting hematocrit below 45% to reduce thrombotic event risk.
5:31: However, it's not just about a single lab value.
5:34: It's about stability over time.
5:36: And with intermittent monitoring and phlebotomy, we may be underestimating how long patients are outside the target level.
5:43: Beyond acute control, other challenges I face are to prevent long-term progression of PV and address the under-recognized burden of chronic iron deficiency.
5:55: In PV we must delicately balance control of disease-related symptoms while minimizing treatment-related toxicity.
6:05: It's really challenging to keep hematocrit consistently below 45%.
6:11: Phlebotomy has long been a cornerstone of treatment in PV, but many patients and physicians struggle with it over time.
6:19: In my opinion, phlebotomy is a waiting to failure approach where we wait for a patient's hematocrit to rise above target and rescue them rather than consistently maintaining optimal disease control.
6:32: Repeated phlebotomies can leave patients dealing with symptomatic iron deficiency in addition to the burden of frequent procedures.
6:42: So what are our other options?
6:43: Cytoreductive therapies are primarily indicated for high risk patients to reduce thrombotic events and control hematocrit below 45%.
6:54: They are an important component of treatment, but they can present challenges.
6:59: Some patients discontinue therapy because of adverse events.
7:03: For example, hydroxyurea may be associated with resistance or intolerance in a subset of patients, and interferons may take several months to achieve their full therapeutic dose.
7:16: A substantial number of patients still spend significant time with uncontrolled hematocrit despite treatment.
7:24: In clinical practice, achieving durable and consistent control can be more challenging than it appears on paper.
7:32: Current treatments may not fully account for symptom burden, iron depletion, adherence challenges, and lifestyle impact.
7:39: Additionally, some therapies may control hematologic parameters without meaningfully improving quality of life.
7:48: Quality of life is an important consideration for these patients.
7:52: They are told at diagnosis that PV is a lifelong struggle with an uncertain course.
7:58: This can create significant anxiety as patients often live with the fear that a serious event could occur at any time.
8:07: While patients may eventually adjust to the diagnosis, many don't adjust to the day to day symptoms.
8:13: It's important to recognize that the burden of PV extends well beyond hematocrit levels.
8:20: We can't focus too narrowly on labs.
8:23: We might achieve the visible goal of hematocrit below 45%, but we often simply exchange the patient's current symptoms and complications with a different set of symptoms and complications.
8:38: Patients with the same diagnosis of PV can experience very different outcomes depending on their symptom burden.
8:45: Symptom burden is not just about discomfort.
8:48: In some MPNs, symptom burden has emerged as a prognostic factor.
8:53: This suggests that symptoms may reflect underlying disease biology, treatment resistance, or complications related to therapy, underscoring the importance of addressing both disease control and quality of life in the management of our patients.
9:10: Despite lasting perceptions of minimal disease burden and PV, nearly 90% of patients reported experiencing symptoms at the time of their diagnosis.
9:20: In an observational study by Poulet et al.
9:23: worsening symptoms affected 47%, or 133 of 285 PV patients in the study, of which the majority were actively treated.
9:34: As you mentioned, Doctor Yacoub, even though phlebotomy remains a common approach for controlling hematocrit, it has its shortcomings.
9:42: We're using an intermittent intervention that may lead to wild swings in hematocrit, which patients then adjust to symptomatically.
9:49: Also intentionally induces iron deficiency.
9:52: Each phlebotomy procedure removes 200 to 250 mg of iron per unit of blood, and about 500 mL of blood, which can significantly worsen iron loss over time.
10:06: That's correct.
10:07: We're exchanging erythrocytosis for symptomatic iron depletion and significant treatment burden.
10:14: When we choose to control hematocrit by deliberately inducing iron deficiency through phlebotomy, we create a global iron deficiency that's a secondary disease we've iatrogenically induced.
10:27: It deprives the brain, heart, and skeletal muscles of iron, inducing muscle weakness, cognitive impairment, and even a syndrome of dementia in some vulnerable elderly patients.
10:41: Patients with PV have dysregulated iron, but what regulates iron in patients without PV?
10:48: Hepcidin has long been recognized as the natural regulator of iron availability to hematopoietic stem cells.
10:55: When functioning properly, it restricts iron from being available to hematopoietic progenitor cells.
11:01: This means iron can continue to remain in the stores available to all the body's organs, but not available to red blood cell production.
11:08: Iron is the rate-limiting factor for red blood cell production.
11:13: In PV though, the disease converts all available iron in the bone marrow niche to a hemoglobin molecule and red blood cells.
11:23: By binding to ferroportin, the body's iron exporter, hepcidin reduces iron release into the plasma, maintaining a feedback loop that limits further absorption.
11:33: Under normal physiology, the hormone hepcidin functions as a regulatory switch that governs iron availability.
11:41: But in PV that regulatory switch is essentially broken. In these patients,
11:46: hepcidin is persistently low, which breaks that natural feedback loop.
11:51: This means that even when systemic iron is scarce, erythropoiesis simply continues in an uncontrolled fashion because the body doesn't get the message.
12:03: Understanding this biological pathway highlights the ultimate therapeutic balance we have long aimed for in PV to uncouple iron stores from red blood cell overproduction, achieving hematocrit control without the collateral damage of global iron deficiency.
12:19: If we can address hepcidin, we may be able to target erythrocytosis at its source.
12:28: As clinicians, we must remember that patients with PV may look well, but are often still symptomatic.
12:35: Fatigue and the subtle effects of chronic iron deficiency can significantly impair quality of life and contribute to long-term complications.
12:44: When making treatment decisions, we need to not just focus on hematocrit control, but also weigh the long-term impact of both the disease and current treatments.
12:55: As we care for patients with PV, we must take a truly global approach.
13:01: Hematocrit control is critical, but we are treating people with cancer, not just cancer in people.
13:09: We cannot ignore the psychological weight of living with a chronic incurable disease that requires lifelong management.
13:17: Mental health and overall well-being must be part of routine care.
13:23: PV is a complex disease that requires an individualized, multi-tool approach.
13:29: We hope that you found today's discussion helpful.
13:32: Thank you for joining us.
Real patient story
Hear a patient discuss their disease journey—from diagnosis and the real-life impact of symptom burden, to navigating the uncertainty that can come with PV.
ViewHide Transcript
0:06: Music has been a part of my life since I was about 4 years old, and the piano is where I pour my soul.
0:12: It's the one thing that I feel like is constant for me.
0:17: I found out that I had PV in March of 2024.
0:24: I didn't know what polycythemia vera was.
0:27: I didn't know what therapeutic phlebotomy was.
0:32: I had started the treatments with one doctor, and then when I went to my new doctor, she didn't see any evidence of PV.
0:42: She also was one of those people who didn't really think that it was anything to worry about.
0:48: So I stopped doing the phlebotomy for several months.
0:51: And I remember calling my doctor and saying, you know, can we just do another blood test?
0:57: When the test came back, it was very evident that I had PV.
1:04: I tend to lose focus kind of easy these days, and I don't really like that.
1:12: I don't like that I feel dizzy a lot.
1:15: I don't like that I have headaches.
1:17: I don't like that I'm tired.
1:19: I lost the ability to do things that had been like breathing for me.
1:25: I have a song that I played on the piano.
1:26: It's my very, very favorite thing to play.
1:29: And it was like I couldn't make the connection between my brain and my fingers.
1:36: I couldn't play it, and it really scared me, and I don't like that I worry about what if it doesn't get better.
1:45: And it's been a long road.
1:48: I've seen situations where people have this and they've gone untreated for way too long. But positively,
1:55: it's given me a freedom to speak out about my health, to make sure that other people understand what PV is.
2:09: I really want anyone who has this to know that it is serious and that there is good information out there about it.
2:18: If someone's doctor is not giving them the information.
2:23: I really want to encourage any patients, and I guess this would go for anybody,
2:29: ask questions,
2:30: find out everything you can
2:33: about whatever it is that your doctor is telling you that you have.
HCT=hematocrit; KOL=key opinion leader; PV=polycythemia vera.
Speak to a representative to discuss diagnosis and treatment considerations in PV
References
1. Verstovsek S, Pemmaraju N, Reaven NL, et al. Real-world treatments and thrombotic events in polycythemia vera patients in the USA. Ann Hematol. 2023;102(3):571-581. doi:10.1007/s00277-023-05089-6. 2. Verstovsek S, Pemmaraju N, Reaven NL, et al. Real-world treatments and thrombotic events in polycythemia vera patients in the USA. Electronic Supplemental Material. Ann Hematol. 2023;102(3):571-581. doi:10.1007/s00277-023-05089-6. 3. Marchioli R, Finazzi G, Specchia G, et al. Cardiovascular events and intensity of treatment in polycythemia vera. N Engl J Med. 2013;368(1):22-33. doi:10.1056/NEJMoa1208500. 4. Poullet A, Busque L, Sirhan S, et al. Symptom burden in myeloproliferative neoplasms: clinical correlates, dynamics, and survival impact—a study of 784 patients from the Quebec MPN research group. Blood Cancer J. 2025;15(1):51. doi:10.1038/s41408-025-01234-8.
5. Randrianarisoa RMF, Ramanandafy H, Mania A, et al. Prevalence and diagnostic performance of iron deficiency in polycythemia. Hematology. 2023;28(1):2204621. doi:10.1080/16078454.2023.2204621. 6. Ginzburg YZ, Feola M, Zimran E, et al. Dysregulated iron metabolism in polycythemia vera: etiology and consequences. Leukemia. 2018;32(10):2105-2116. doi:10.1038/s41375-018-0207-9. 7. Vainchenker W, Kralovics R. Genetic basis and molecular pathophysiology of classical myeloproliferative neoplasms. Blood. 2017;129(6):667-679. doi:10.1182/blood-2016-10-695940. 8. Kuykendall AT, Fine JT, Kremyanskaya M. Contemporary challenges in polycythemia vera management from the perspective of patients and physicians. Clin Lymphoma Myeloma Leuk. 2024;24(8):512-522. doi:10.1016/j.clml.2024.04.003. 9. Data on file. Takeda Pharmaceuticals U.S.A., Inc. 10. Tefferi A, Barbui T. Polycythemia vera: 2024 update on diagnosis, risk-stratification, and management. Am J Hematol. 2023;98(9):1465-1487. doi:10.1002/ajh.27002. 11. Zhao ZJ, Vainchenker W, Krantz SB et al. Role of tyrosine kinases and phosphatases in polycythemia vera. Semin Hematol. 2005;42(4):221-229. doi:10.1053/j.seminhematol.2005.05.019. 12. Ling B, Xu Y, Qian S, et al. Regulation of hematopoietic stem cells differentiation, self-renewal, and quiescence through the mTOR signaling pathway. Front Cell Dev Biol. 2023;11:1186850. doi:10.3389/fcell.2023.1186850. 13. Waggoner M. Polycythemia vera: thinking beyond the hematocrit. J Adv Pract Oncol. 2023;14(5):405-413. doi:10.6004/jadpro.2023.14.5.5. 14. Griesshammer M, Kiladjian JJ, Besses C. Thromboembolic events in polycythemia vera. Ann Hematol. 2019;98(5):1071-1082. doi:10.1007/s00277-019-03625-x. 15. MPN Research Foundation. Polycythemia vera (PV). Updated 2026. Accessed June, 2026. Available at: https://mpnresearchfoundation.org/polycythemia-vera-pv/. 16. Lichtman MA, Kaushansky K, Prchal JT, Levi MM, Burns LJ, Linch DC, eds. Polycythemia vera. In: Williams Manual of Hematology. 10th ed. McGraw Hill; 2022:248-253. 17. Blood Cancer United. Myeloproliferative neoplasms: in detail. Revised 2025. Accessed June, 2026. Available at: https://bloodcancerunited.org/. 18. National Organization for Rare Disorders (NORD). Polycythemia vera. Revised March, 2026. Accessed June, 2026. Available at: https://rarediseases.org/rare-diseases/polycythemia-vera/. 19. Cuthbert D, Stein BL. Polycythemia vera-associated complications: pathogenesis, clinical manifestations, and effects on outcomes. J Blood Med. 2019;10:359-371. doi:10.2147/JBM.S189922. 20. Brabrand M, Frederiksen H. Risks of solid and lymphoid malignancies in patients with myeloproliferative neoplasms: clinical implications. Cancers. 2020;12(10):3061. doi:10.3390/cancers12103061. 21. Landtblom AR, Bower H, Andersson TML, et al. Second malignancies in patients with myeloproliferative neoplasms: a population-based cohort study of 9,379 patients. Leukemia. 2018;32(10):2203-2210. doi:10.1038/s41375-018-0027-y. 22. Mesa R, Miller CB, Thyne M, et al. Myeloproliferative neoplasms (MPNs) have a significant impact on patients' overall health and productivity: the MPN Landmark survey. BMC Cancer. 2016;16:167. doi:10.1186/s12885-016-2208-2. 23. Mesa RA, Miller CB, Thyne M, et al. Differences in treatment goals and perception of symptom burden between patients with myeloproliferative neoplasms (MPNs) and hematologists/oncologists in the United States: findings from the MPN Landmark survey. Cancer. 2017;123(3):449-458. doi:10.1002/cncr.30325. 24. National Cancer Institute. Coping with cancer: emotions and cancer. Updated April, 2025. Accessed June, 2026. Available at: https://www.cancer.gov/about-cancer/coping/feelings. 25. Bradford A, Young K, Whitechurch A, et al. Disabled, invisible and dismissed—the lived experience of fatigue in people with myeloproliferative neoplasms. Cancer Rep (Hoboken). 2023;6(1):e1655. doi:10.1002/cnr2.1655. 26. Verstovsek S, Harrison CN, Kiladjian JJ, et al. Markers of iron deficiency in patients with polycythemia vera receiving ruxolitinib or best available therapy. Leuk Res. 2017;56:52-59. doi:10.1016/j.leukres.2017.01.032. 27. Mesa RA, Schwager S, Radia D, et al. The Myelofibrosis Symptom Assessment Form (MFSAF): an evidence-based brief inventory to measure quality of life and symptomatic response to treatment in myelofibrosis. Leuk Res. 2009;33(9):1199-1203. doi:10.1016/j.leukres.2009.01.035. 28. Grunwald MR, Burke JM, Kuter DJ, et al. Symptom burden and blood counts in patients with polycythemia vera in the United States: an analysis from the REVEAL study. Clin Lymphoma Myeloma Leuk. 2019;19(9):579-584.e1. doi:10.1016/j.clml.2019.06.001. 29. Barbui T. Appropriate management of polycythemia vera with cytoreductive drug therapy: European LeukemiaNet 2021 recommendations. Hematol Transfus Cell Ther. 2022;44(1):S3-S4. doi:10.1016/j.htct.2022.09.1190. 30. Landolfi R, Marchioli R, Kutti J, et al. Efficacy and safety of low-dose aspirin in polycythemia vera. N Engl J Med. 2004;350(2):114-124. doi:10.1056/NEJMoa035572. 31. Tefferi A, Vannucchi AM, Barbui T. Polycythemia vera: historical oversights, diagnostic details, and therapeutic views. Leukemia. 2021;35(12):3339-3351. doi:10.1038/s41375-021-01401-3.
32. Visweshwar N, Fletcher B, Jaglal M, et al. Impact of phlebotomy on quality of life in low-risk polycythemia vera. J Clin Med. 2024;13(16):4952. doi:10.3390/jcm13164952. 33. Silver RT, Abu-Zeinah G. Polycythemia vera: aspects of its current diagnosis and initial treatment. Expert Rev Hematol. 2023;16(4):253-266. doi:10.1080/17474086.2023.2198698. 34. Kim KH, Oh KY. Clinical applications of therapeutic phlebotomy. J Blood Med. 2016;7:139-144. doi:10.2147/JBM.S108479. 35. Edahiro Y, Komatsu N. Iron deficiency and phlebotomy in patients with polycythemia vera. Int J Hematol. 2025;121(1):39-44. doi:10.1007/s12185-024-03868-z. 36. Bennett C, Jackson VE, Pettikiriarachchi A, et al. Iron homeostasis governs erythroid phenotype in polycythemia vera. Blood. 2023;141(26):3199-3214. doi:10.1182/blood.2022016779. 37. Assi TB, Baz E. Current applications of therapeutic phlebotomy. Blood Transfus. 2014;12 (Suppl 1):s75-83. doi:10.2450/2013.0299-12. 38. Mayo Clinic. Hydroxyurea (oral route). Updated March, 2026. Accessed June, 2026. Available at: https://www.mayoclinic.org/drugs-supplements/hydroxyurea-oral-route/description/drg-20068109. 39. Parasuraman S, DiBonaventura M, Reith K, et al. Patterns of hydroxyurea use and clinical outcomes among patients with polycythemia vera in real-world clinical practice: a chart review. Exp Hematol Oncol. 2016;5:3. doi:10.1186/s40164-016-0031-8. 40. Alvarez-Larrán A, Pereira A, Cervantes F, et al. Assessment and prognostic value of the European LeukemiaNet criteria for clinicohematologic response, resistance, and intolerance to hydroxyurea in polycythemia vera. Blood. 2012;119(6):1363-1369. doi:10.1182/blood-2011-10-387787. 41. Jakafi (ruxolitinib). Package insert. Incyte Corporation; 2023. 42. BESREMi (ropeginterferon alfa-2b-njft). Package insert. PharmaEssentiaⓇ USA Corporation; 2024. 43. Vachhani P, Mascarenhas J, Bose P, et al. Interferons in the treatment of myeloproliferative neoplasms. Ther Adv Hematol. 2024;15:1-22. doi:10.1177/20406207241229588. 44. Tremblay D, Ronner L, Podoltsev N, et al. Ruxolitinib discontinuation in polycythemia vera: patient characteristics, outcomes, and salvage strategies from a large multi-institutional database. Leuk Res. 2021;109:106629. doi:10.1016/j.leukres.2021.106629. 45. Chamseddine RS, Savenkov O, Rana S. Cytoreductive therapy in younger adults with polycythemia vera: a meta-analysis of safety and outcomes. Blood Adv. 2024;8(10):2520-2526. doi:10.1182/bloodadvances.2023012459. 46. Abelsson J, Andréasson B, Samuelsson J, et al. Patients with polycythemia vera have worst impairment of quality of life among patients with newly diagnosed myeloproliferative neoplasms. Leuk Lymphoma. 2013;54(10):2226-2230. doi:10.3109/10428194.2013.766732. 47. American Cancer Society. Adjusting to life with cancer. Updated December, 2025. Accessed June, 2026. Available at: https://www.cancer.org/cancer/coping/adjusting-to-life-with-cancer.html. 48. Ponce RKM, Verma K, Gergen-Barnett K, et al. A review of medical mistrust across the cancer continuum of care and current interventions. J Community Health. 2025;50(4):750-760. doi:10.1007/s10900-025-01462-w. 49. Poullet A, Busque L, Sirhan S, et al. Symptom burden in myeloproliferative neoplasms: clinical correlates, dynamics, and survival impact—a study of 784 patients from the Quebec MPN Research Group. Supplemental Figure 1. Blood Cancer J. 2025;15:51. doi:10.1038/s41408-025-01234-8. 50. Handa S, Ginzburg Y, Hoffman R, et al. Hepcidin mimetics in polycythemia vera: resolving the irony of iron deficiency and erythrocytosis. Curr Opin Hematol. 2023;30(2):45-52. doi:10.1097/MOH.0000000000000747. 51. McFarland DC, Shaffer KM, Polizzi H, et al. Associations of physical and psychologic symptom burden in patients with Philadelphia chromosome-negative myeloproliferative neoplasms. Psychosomatics. 2018;59(5):472-480. doi:10.1016/j.psym.2018.01.006. 52. Yu J, Parasuraman S, Paranagama D, et al. Impact of myeloproliferative neoplasms on patients' employment status and work productivity in the United States: results from the living with MPNs survey. BMC Cancer. 2018;18:420. doi:10.1186/s12885-018-4322-9. 53. National Institutes of Health (NIH). Talking to your doctor. Updated March, 2025. Accessed June, 2026. Available at: https://www.nih.gov/institutes-nih/nih-office-director/office-communications-public-liaison/clear-communication/talking-your-doctor-or-health-care-provider. 54. Harrison CN, Ross DM, Fogliatto LM, et al. Patient and physician perceptions regarding treatment expectations and symptomatology in polycythemia vera: insights from the Landmark 2.0 global health survey. Hemasphere. 2025;9(3):e70106. doi:10.1002/hem3.70106. 55. Manz K, Heidel FH, Koschmieder S, et al. Comparison of recognition of symptom burden in MPN between patient- and physician-reported assessment—an intraindividual analysis by the German Study Group for MPN (GSG-MPN). Leukemia. 2025;39(4):864-875. doi:10.1038/s41375-025-02524-7. 56. Emanuel RM, Dueck AC, Geyer HL, et al. Myeloproliferative neoplasm (MPN) symptom assessment form total symptom score: prospective international assessment of an abbreviated symptom burden scoring system among patients with MPNs. J Clin Oncol. 2012;30(33):4098-103. doi:10.1200/JCO.2012.42.3863. 57. Almeida LR, Faustino D, Gameiro R, et al. Masked polycythemia vera and iron deficiency in a fertile-age woman. Cureus. 2023;15(1):e33545. doi:10.7759/cureus.33545. 58. Saad HKM, Abd Rahman AA, Ab Ghani AS, et al. Activation of STAT and SMAD signaling induces hepcidin re-expression as a therapeutic target for β-thalassemia patients. Biomedicines. 2022;10(1):189. doi:10.3390/biomedicines10010189. 59. Pilo F, Angelucci E. Vamifeport: monography of the first oral ferroportin inhibitor. J Clin Med. 2024;13(18):5524. doi:10.3390/jcm13185524. 60. Ganz T. Hepcidin—a regulator of intestinal iron absorption and iron recycling by macrophages. Best Pract Res Clin Haematol. 2005;18(2):171-182. doi:10.1016/j.beha.2004.08.020. 61. Cleveland Clinic. Iron-deficiency anemia. Revised December, 2024. Accessed June, 2026. Available at: https://my.clevelandclinic.org/health/diseases/22824-iron-deficiency-anemia. 62. Faruqi A, Zubair M, Mukkamalla SKR. Iron-binding capacity. In: StatPearls. Treasure Island (FL): StatPearls Publishing; May 2, 2024.